Lung cancer accounts for one in five deaths worldwide. The past few years have seen considerable advances in treatment for lung cancer, yet the prognosis remains low. Lung cancer causes symptoms that come up late in the course of the disease and assessments are complicated. This means that half of the patients have a spread disease at diagnosis.
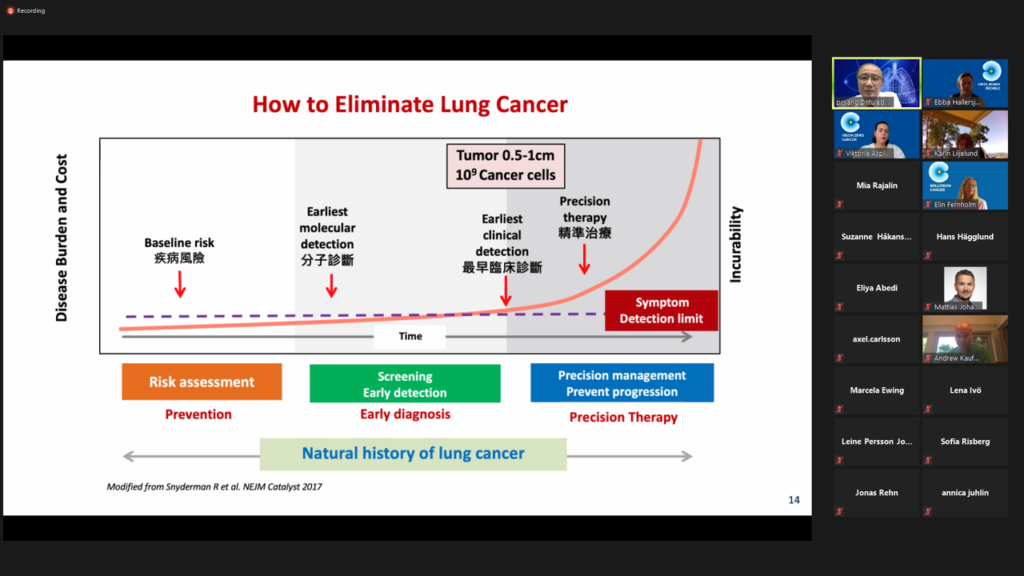
Early detection and prevention are the best strategies to improve the treatment outcome or eliminate the disease. People who smoke or have smoked have the greatest risk of lung cancer, though lung cancer also increasingly occurs in people who have never smoked. Lung cancer in never-smokers is a global rising concern and there is a fast growing need to understand how never-smokers’ disease differs from that of smokers, and how to effectively prevent and diagnose it early.
Vision Zero Cancer therefore invited participants ranging from current leading researchers in the field and clinicians to patient representatives and the medical industry to share experience and discoveries on how to develop an effective preventive strategy and opportunities for screening.
The meeting held around 30 participants and keynote speaker was Dr. Pan-Chyr Yang (MD, PhD, Chair Professor at the National Taiwan University Hospital and Academician of Academia Sinica, Taiwan). Dr. Yang shared the findings of the Taiwan Lung Cancer Screening for Never-Smoker Trial (TALENT), a nationwide lung cancer low-dose CT screening study focused on never-smokers which also aims to develop an effective strategy for screening of lung cancer in never-smokers and establish a risk prediction model to identify high-risk population that may benefit from low-dose CT screening. In Taiwan, lung cancer is the leading cause of cancer mortality, and 53% of those who have died of lung cancer were never-smokers. The US National Lung Cancer Screening Trial (NLCST) and the Dutch NELSON trials demonstrated that the use of low-dose CT is effective for lung cancer screening; however, most of the lung cancer screenings focused on heavy smokers.
Of the 12,011 individuals included in the trial, the prevalence of lung cancer was 3.2% and 2.0% in participants with and without lung cancer family history, respectively. As explained during the meeting by Dr. Yang, 96.5% of the detected patients were stage 0 or 1 and potentially curable by surgery. The study also demonstrated the high risk of family history, especially among participants with a first-degree family history of lung cancer.The meeting further contained a panel discussion where Andrew Kaufman (MD, Associate Professor, thoracic surgeon at Mount Sinai Hospital in New York City) Kersti Oselin (MD, PhD, Medical Oncologist, North-Estonian Regional Hospital Cancer Center) Marcela Ewing (MD, PhD, Specialist Oncology and General Medicine, Sahlgrenska Academy, Regional Lead Early Detection of Cancer, Confederation of Regional Cancer Centres) Mattias Johansson (PhD, Scientist, Genetic Epidemiology Group, International Agency for Research on Cancer (IARC), World Health Organization) and Mikael Johansson (MD, Associate Professor, Senior Consultant Oncology, Umeå University Hospital and Senior lecturer at Umeå University, Chair of the National Working Group for Lung Cancer Care) together with Dr. Pan-Chyr Yang elaborated their thoughts on the findings of the TALENT-study and how this relates to what they are facing in their current work.
Andrew Kaufman who is the leader of the never-smoking initiative at Mount Sinai Hospital, New York, reflected that caring for never-smoking lung cancer patients comes down to the intersection between epidemiology, biology, clinical capability, precision medicine, surgical care and all other clinical attributes available. He put emphasis on that it takes a multidisciplinary approach to look at the data and find out what is the substrate we are dealing with in terms of a clinical population, while also stating that for most cancers unfortunately the time for best intervention is at an asymptomatic time point. Dr. Kaufman continued by being hopeful that discussions like the one this meeting facilitated will shed light on and give direction to find the right thread to start pulling on to make a difference in the case of lung cancer. By learning from the important findings of Dr. Yangs work we will be able to provide ways to be smarter at identifying patients at risk yet also not increasing the costs of the inefficiency of care.
The various competent outlooks and insights presented by the panel gave a good transition to the last part of the meeting where Mattias Johansson from the Genetic Epidemiology Group at the WHO International Agency for Research on Cancer (IARC) presented a proof on concept study on the use of biomarkers to improve early detection and the possibilities this presents to detect more lung cancer patients in time. Medical oncologist Kersti Oselin from the North-Estonian Regional Hospital Cancer Center gave insights on AI for early detection and the prognostic significance of genomic markers in lung cancer recurrence. Rounding up the meeting from London Amied Shamaan, director within AI and clinical collaboration presented the work of a collaboration between Oxford University and GE Healthcare with other industry partners in a consortium that is formed around lung cancer screening and innovation and goes under the name of The Integration and Analysis of Data using Artificial Intelligence to Improve Patient Outcomes with Thoracic Diseases (DART). The consortium has come together to be agile around the lung cancer screening process in the UK to provide innovation in technology and to be able to involve and better affect the patient population.
During the autumn follow-up meetings will be held to dig deeper into the common areas and challenges facing early detection of never smokers. Leveraging clearly on the consensus of the meeting around the need to gather across professions and sectors to build momentum around who and how to find never-smoking lung cancer patients at the right time.
The purpose of this meeting was to share discoveries and experience on how to develop an effective preventive strategy.
How do we detect cancer earlier?
The earlier cancer is detected, the greater are the chances of survival. With new systems and knowledge, we can pick up on symptoms earlier and more quickly come to treatment. And get more chances to reach the vision of zero people dying from cancer and more people living longer and better.