Home”Breaking new ground on all fronts” – Oncology in Sweden about Vision Zero Cancer
”Breaking new ground on all fronts” – Oncology in Sweden about Vision Zero Cancer
In the latest issue of Oncology in Sweden, a number of people from Vision Zero Cancer were interviewed about the beginning, the vision, how it is going to become reality and the importance of collaboration and inclusiveness to make a change.
“Our vision is that no one should have to die from cancer in Sweden and the goal of our unusual collaboration is to investigate what we need to do to reach it.”
The journalist Evelyn Pesikan talked to several members of the core team about their roles and hopes for Vision Zero Cancer. But also about hands-on actions and forms of collaboration.
Vision Zero Cancer challenges the prevailing ecosystem and connects new ones. We are going to turn cancer from a deadly into a curable or chronic disease.
HomeResearcher studies Vision Zero Cancer for future innovation
Researcher studies Vision Zero Cancer for future innovation
Are milieus like Vision Zero Cancer a good way to accelerate innovation? At Stockholm School of Economics, doctoral student John-Erik Bergkvist is researching this – the methodology for building a vision-driven innovation milieu.
John-Erik Bergkvist, PhD student at House of Innovation, Stockholm School of Economics
Vision Zero Cancer aims to be an innovation milieu that engages actors from different sectors and disciplines to achieve a common vision: that no one should have to die of cancer. The phenomenon of vision-driven innovation milieus is not new – but there is not much research on it, yet. Doctoral student John-Erik Bergkvist, at House of Innovation, Stockholm School of Economics, is working on changing that. “Vision Zero Cancer is an exciting organization,” he says. “They are based on a call from The Swedish Innovation Agency, Vinnova, around vision-driven health. Based on ideas that innovation can be accelerated through cooperation and a clear direction.”
It is based on the idea that it’s rarely one actor that accounts for the entire value. In the case of cancer care, there are many actors. The pharmaceutical industry, the medtech industry, doctors, nurses, IT-functions – all that is required for good cancer care. The idea is that these actors should not innovate individually but explore joint missions in a broader ecosystem.
Previous research has mainly focused on collaborations between organizations or ways of coordinating ecosystems that are centered around a certain product. Vision Zero Cancer is more about creating an arena and conditions for long-term dialogue – so that collaboration becomes natural. Preferably in slightly unexpected constellations. “Theoretically, it’s about changing informal and formal institutions. The assumption in Vinnova’s call is that broad arenas for knowledge exchange can give birth to new ideas and increase innovation capacity in the ecosystem as a whole.”
Words such as cross-sectoral, cross-disciplinary, flexible, and dynamic permeate the call. “It is based on the idea that it’s rarely one actor that accounts for the entire value. In the case of cancer care, there are many actors. The pharmaceutical industry, the medtech industry, doctors, nurses, IT-functions – all that is required for good cancer care. The idea is that these actors should not innovate individually but explore joint missions in a broader ecosystem. And try to get the ecosystem to bring about system transformation.”
Healthcare is more than just the treatment itself; it is also a matter of organizing to carry out the treatment. In which knowledge of how to do it effectively is needed.
John-Erik Bergkvist will follow how Vision Zero Cancer is built up and received, which drivers and hindering factors there are. A longitudinal case study. This will be the theme of one of the articles in his doctoral thesis, which usually contains four to five articles. “The rest is made up of experimental studies around what factors matters to those who are going to engage with the ecosystem, how innovative ability is affected by education and how receptive different professions are to the ideas of other professions”
The fact that Vision Zero Cancer is an innovation milieu within healthcare was something that attracted John-Erik Bergkvist, who has experience within healthcare from before. His CV includes positions as an analyst at the Swedish Agency for Health and Social Care Analysis and analyst at the Swedish Government Offices’ writing an Official Government report on the subject ‘The future specialist nurse – new role, new opportunities’. He is well versed in the challenges facing healthcare. Organization is one of them. “Healthcare is more than just the treatment itself; it is also a matter of organizing to carry out the treatment. In which knowledge of how to do it effectively is needed.”
There is certainly scepticism about initiatives perceived as “external” fabrications. However, Vision Zero cancer exhibits characteristics that are beneficial. They consist of a wide mix of people “from within” healthcare. And not only from the profession, but also patients, the pharmaceutical industry and the medtech industry
By studying Vision Zero Cancer and the conditions for innovation, John-Erik Bergkvist hopes to be able to generate knowledge about its way of organizing and draw general conclusions that can be used for similar milieus. To learn if vision-driven innovation environments are something for the future. In this he is supervised by Associate Professor Anna Essén. “John-Erik’s research contributes to the vision by critically reviewing what Vision Zero Cancer actually does. Sometimes you don’t do what you think you’re doing. It increases Vision Zero Cancer’s own ability to reflect and thus the capacity to adapt, improve, and achieve its goals.
Anna Essén, assistant professor at House of Innovation, Stockholm School of Economics
Anna Essén points out that innovation milieus are nothing new but have existed in different contexts in the past. With varied results. “There is certainly scepticism about initiatives perceived as “external” fabrications. However, Vision Zero cancer exhibits characteristics that are beneficial. They consist of a wide mix of people “from within” healthcare. And not only from the profession, but also patients, the pharmaceutical industry and the medtech industry.”
Vision Zero Cancer matches actors with complementary ideas – it thereby reduces transaction costs and allows actors to leverage their investments. No one can build a complete solution for a transformation of cancer care themselves. A viable approach is therefore to enable actors to combine and recombine their nisched ideas and offerings with other’s contributions. I think Vision Zero Cancer is making a difference here already – by facilitating such combinations.
The network of actors is something that Anna Essén sees as a strength. “Vision Zero Cancer matches actors with complementary ideas – it thereby reduces transaction costs and allows actors to leverage their investments. No one can build a complete solution for a transformation of cancer care themselves. A viable approach is therefore to enable actors to combine and recombine their nisched ideas and offerings with other’s contributions. I think Vision Zero Cancer is making a difference here already – by facilitating such combinations.”
Vision Zero Cancer challenges the prevailing ecosystem
Fewer people shall get ill and die from cancer. For that to work, we need to think in new ways. Both in terms of developing new solutions and getting better at using what is available.
HomeSweden-Russia experience exchange on lung cancer – accelerating innovation to improve survival and quality of life for people with lung cancer
Sweden-Russia experience exchange on lung cancer – accelerating innovation to improve survival and quality of life for people with lung cancer
Around 60 experts gathered during the virtual experience exchange between Sweden and Russia as part of a collaboration between the Association of Oncologists of Russia and Vision Zero cancer, aided by Business Sweden and the Embassy of Sweden to the Russian Federation.
A warm and shared welcome to the meeting was given by H.E. Malena Mård, Ambassador of Sweden to the Russian Federation, Mattias Lindgren, Swedish Trade Commissioner to the Russian Federation, Market Area Director Eurasia, Business Sweden, Professor Andrey Kaprin, MD, General Director of the National Medical Research Radiological Center of the Ministry of Health of the Russian Federation, President of the Association of Oncologists of Russia, and Ebba Hallersjö Hult, Head of Vision Zero Cancer. The scene for Cancer care in Russia and Sweden with particular focus on lung cancer was set by presentations from Professor Andrey Ryabov, MD, Deputy General Director of the National Medical Research Radiological Center of the Ministry of Health of the Russian Federation and Associate Professor Mikael Johansson, MD, Senior Consultant Oncology, Umeå University Hospital and Senior lecturer at Umeå University.
The presentations and following discussions centred around three key areas containing an impressive 25 expert speakers giving their view on (1) Prevention, Improved awareness and Education, (2) Early Detection and Screening and(3) Diagnostics, Treatment and Care.
Attached to this short overview is the full agenda.
The meeting has further underbuilt the coming memorandum of cooperation (MoC) between the National Medical Research Radiological Centre of the Ministry of Health of the Russian Federation (NMRRC), the Association of Oncologists of Russia (AOR) and Vision Zero Cancer as well as paved way for experience exchanges on site in Sweden and Russia. All to continue the common fight against cancer.
The purpose of this meeting was to share knowledge and experience on how to improve early cancer diagnosis, outcomes and care for patients and to discuss potential new technologies for early lung cancer detection, including the implementation of targeted screening and precision diagnostics and treatment.
Five different areas that need renewal
Fewer people shall get ill and die from cancer. For that to work, we need to think in new ways. Both in terms of developing new solutions and getting better at using what is available.
HomePrecision medicine improves cancer care and makes it more equitable and efficient
Precision medicine improves cancer care and makes it more equitable and efficient
One size fits all is no longer applicable. Precision medicine has made several advancements in recent years. Rapid development in research and technology is creating conditions for a transformation of the system. With these developments come challenges and consequences – but which ones? And what exactly is accommodated within the concept of precision medicine? These questions where discussed among 60 participants at a digital round table recently hosted by Vision Zero Cancer and the Confederation of Regional Cancer Centers.
Many precision medicine initiatives are underway. In order to gather the scope of initiatives in Sweden, recapture the state of knowledge and sharpen collaboration, Vision Zero Cancer and the Confederation of Regional Cancer Centers extended invitations to a digital round table. Among the participants were representatives from healthcare, patient associations authorities, industry, academia and other experts.
So what is precision medicine? Precision medicine is about tailoring healthcare for a subgroup of patients. Based on genetics, environment and lifestyle factors, diagnostics, treatments, and decisions can be improved and become more precise. These include molecular biology, genetic sequencing, new imaging techniques, gene therapy, AI, machine learning and data management.
David Gisselsson Nord, MD, PhD, Professor and Specialist Physician, Senior Consultant in molecular pathology in the Southern Healthcare Region, gave examples from the reality of genetic sequencing in childhood cancer. – Precision diagnostics will be of great benefit to many, says Dr. Gisselsson Nord, but he also points out that sometimes it only works for a certain period of time. We cannot have a static treatment when cancer is ever changing by nature.
Advancements in liquid biopsies, AI, blood tests and national collaborations
Richard Rosenquist Brandell, MD, PhD, Professor of clinical genetics at Karolinska Institutet and Senior Physician at Karolinska University Hospital, gave insights about the Swedish national collaboration Genomic Medicine Sweden (GMS), where he is chairman. GMS coordinates the introduction of precision medicine nationwide, with centers at the seven university hospitals and has launched a national genomics platform to share data across the country. – We develop standards of how to analyze and interpret, how to work with precision diagnostics and build teams at each center that can use it in treatment. At the same time, it will be a good resource for research and innovation as we can collect the entire country’s data.
AI can improve the operational steps we already have today, rebuild workflows and, not least, do things that we couldn’t do before. Like predicting certain progress. But this also means that new competences in healthcare are needed, such as computer scientists.
Fredrik Enlund, Associate Professor of molecular pathology and head of the Centre for Diagnostics at Region Kalmar, talked about liquid biopsies, a special sampling that can capture the heterogeneity of tumors. That is, genetic clones and mutations within the same tumor. – Heterogenous tumors are a challenge – which clone is to be primarily treated and what do we do when the patient has received targeted treatment but has developed a clone that can resist the primary treatment? This is where we benefit from liquid biopsies. They can capture that heterogeneity and reduce the risk of resistance if the disease develops. Liquid biopsies can also be used in hard-to-reach tumors to find the right treatment.
The possibilities that comes with AI are great for precision medicine, says Claes Lundström, Adjunct Professor at Linköping University and research director at Sectra. It can save a lot of time for those who work in healthcare and save lives. – AI can improve the operational steps we already have today, rebuild workflows and, not least, do things that we couldn’t do before. Like predicting certain progress. But this also means that new competences in healthcare are needed, such as computer scientists.
Peter Nygren, MD, PhD, Senior Consultant and Professor of cancer pharmacology at Uppsala University and national coordinator of the MEGALiT project told us about the national cross-sectoral collaboration that under controllable conditions implement new ways of working within oncology. – We will test tumor response, feasibility and safety of different drugs on different diagnoses, says Dr. Nygren. It paves the way for more advanced use of precision medicine in the next step.
There are certain crossroads in life where you meet healthcare providers. At the childcare center, at school related health services or in screening programs. While being in contact with healthcare, you could easily add taking a blood test to find biomarkers for cancer. Maybe the end goal could even be a simplified blood test to be taken home?
Precision medicine can also make it possible to earlier on detect diseases and find their predispositions. Beatrice Melin, MD, PhD, Senior Consultant and Professor at the Department of Radiation Sciences at Umeå University, pointed out that simple blood tests can provide many answers. – There are certain crossroads in life where you meet healthcare providers. At the childcare center, at school related health services or in screening programs. While being in contact with healthcare, you could easily add taking a blood test to find biomarkers for cancer. Maybe the end goal could even be a simplified blood test to be taken home?
Authorities investigate the impact and benefits of precision medicine
The roundtable also offered an update from Swedish authorities on their ongoing investigations. Johan Strömblad, Project Manager at the Swedish Agency for Health and Care Services Analysis, talked about the impact of precision medicine on healthcare. – Achieving the vision requires political priorities, resources to make necessary transitions, patient participation, integration of research and clinical practice, and health data amongst other things. We need to ask questions of how we further cross-sectoral development within knowledge management in the organization, what boundaries are applicable to national highly specialized care and which staff need what knowledge.
As treatments become more individualized for each patient, how do we evaluate the societal benefits of treatment?
Anna Alassaad, Pharmacist, and Project Manager at the Dental and Pharmaceutical Benefits Agency, reported on the health economic assessments for precision medicine – how payment models can be developed to address the high costs of treatment and uncertainties. – As treatments become more individualized for each patient, how do we evaluate the societal benefits of treatment? This is one of the themes within the analysis. Another theme is value – precision medicine comes with new possibilities, such as earlier risk identification and possible cure. Are values such as these captured in traditional health economic analyses?
Several collaborative projects are developing precision medicine in cancer
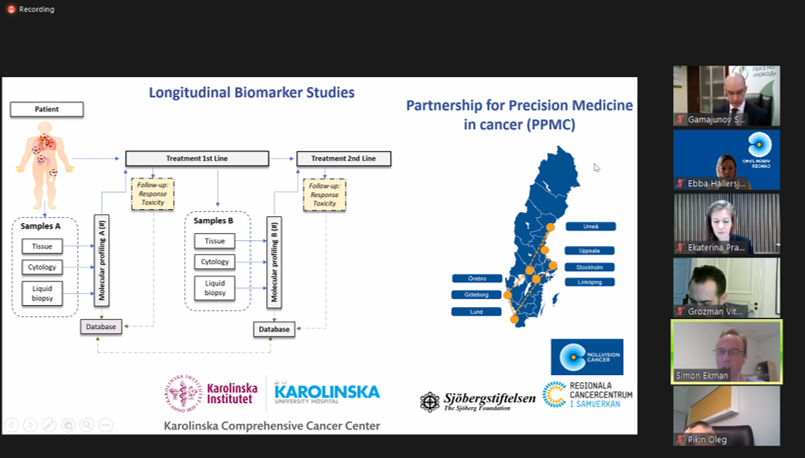
Simon Ekman, MD, PhD, Senior Consultant and Associate Professor of oncology at Karolinska University, talked about the Partnership for Precision Medicine in Cancer (PPMC) – an initiative to strengthen Swedish translational research on precision medicine, with coordination of biobanking, clinical data and research data from patients. PPMC is a virtual organization with regional nodes in University hospitals and regional cancer centers. – We want to achieve better precision in treatments, facilitate follow-ups and find new therapies, says Simon Ekman.
Work at the local level is essential for things to happen on the floor. It’s about building understanding among managers and employees about what precision medicine is. New ways of working are necessary and so is applying new ways of thinking about organization. Academia needs to become a clearer part of healthcare.
Anna Martling, MD, PhD, Professor of Surgery, Senior Consultant at Karolinska University Hospital and Dean of Campus North of Karolinska Institutet, leads the Taskforce for accelerated development of precision medicine. The goal is to accelerate development and coordinate activities within the Stockholm Region by working for implementation in healthcare in order for patients to reap the benefits. – Work at the local level is essential for things to happen on the floor, Dr. Martling says. It’s about building understanding among managers and employees about what precision medicine is. New ways of working are necessary and so is applying new ways of thinking about organization. Academia needs to become a clearer part of healthcare.
We want to achieve better precision in treatments, facilitate follow-ups and find new therapies
The collaboration program of Health & Life Science is based on the Swedish Life Science strategy. Among other things, it states that Sweden should be a leader in the introduction of precision medicine. Frida Lundmark from The Research based Pharmaceutical Industry is coordinating the government’s liaison group around precision medicine. – We’re going to act like the glue holding everything together. We won’t identify or initiate our own initiatives, but rather help and highlight the regional initiatives that are underway and further their conditions towards national dissemination and implementation, says Frida Lundmark. We will also structure proposals for the Government Offices of Sweden based on what is already initiated adding extra muscle and speed to enforcement.
Break-out groups provided input for further analysis
The 60 participants were towards the last hour divided into groups to discuss questions about what efforts will be required in the coming years for precision medicine to ensure good, equitable and effective cancer care, as well as which constellations of actors are needed to achieve this. Each group had been appointed a theme to give lead to the discussions, the themes ranged between technology, clinical trials and policy development.
Among the answers where proposals to standardize and coordinate payment models, data sharing and guidelines nationally. Many pointed to the importance of developing competence for existing staff within precision medicine, but also the need to introduce completely new competences and trainings. Several mentioned that the need, value and effects of different therapies, medicines and health economics must be evaluated. The proposals also touched upon increased understanding of the value of investing in research and placing Sweden on the international map. Further we need to get better at finding and involving patients in order for precision medicine to benefit those intended.
The result of the workshop will be part of the foundation for further work by Vision Zero Cancer and the Confederation of Regional Cancer Centers. It is hoped that these valuable insights can serve as starting points in further analyses and collaborations on various issues.
Thank you to all participants!
Better treatment, better lives
Chemotherapy also gives way to healthy cells. We want to find more precise treatment, focusing on the goal and on providing as little side effects as possible. Both during and after treatment. Because it is not just about survival, it is about continuing to live.
The earlier cancer is detected, the greater are the chances of survival. With new systems and knowledge, we can pick up on symptoms earlier and more quickly come to treatment.
HomeHow Sweden will become a global leader yet again
How Sweden will become a global leader yet again
More and more patients need radiotherapy. But radiation therapy treatment is an area where research in Sweden has gone from leading to lagging behind internationally. How do we reverse the trend? How do we ensure that radiation therapy research continues to develop and become evenbetter so that more patients survive and can live a better life with less side effects?
Kjell Bergfeldt, MD, PhD. Foto: Staffan Claesson
Sweden was for a long time a leader in the field of radiation therapy research. But in the last 20 years we have been falling behind – fever scientific articles are published, less money goes towards research and people who hold it as an occupation are getting more scarce. Kjell Bergfeldt, MD, PhD, with more than twenty years of experience as an oncologist has the task of developing Swedish radiation therapy and is working to change all of this. – Half of all cancer patients are estimated to receive radiotherapy at some point during their illness. Developed radiation therapy can improve the lives of many people.
Innovations such as the MRI camera and PET scanning have made the images sharper and more detailed. Treatment planning programmes have been developed to make radiation therapy more precise. Dr Bergfeldt sees it as a form of precision therapy where artificial intelligence and machine learning can help improve treatment further. – In the past, we had to include space for uncertainty in the planning which meant that the volumes that were irradiated could become large and cause severe side effects. With better images and software, we have improved radiation therapy treatment and there are great opportunities to improve it further. If we can isolate the area of the tumor better, it may be possible to increase the dose. As long as there is a risk of hitting healthy organs, we want to keep the dose down.
– Half of all cancer patients are estimated to receive radiotherapy at some point during their illness. Developed radiation therapy can improve the lives of many people.
For lung cancer there is a particular challenge. – The brain is located in an exact place. The part that the radiation is aimed to hit is still. But the lungs move with your breathing. Therefore, the tumor is moving. How do you beam on a moving organ? The technology to do so has evolved rapidly but yet it is not fully implemented everywhere.
The fact that the technology has become more advanced has also made the management of it more complicated within healthcare. This leaves one more thing that must be developed. Competence. – The number of patients receiving radiation treatment is constantly increasing. However, the number of nurses and doctors who can master the increasingly complex technology and who are doing research in the field is not increasing at the same rate. In order to provide the best treatment, we need to attract more doctors, nurses and medical physicists who are focused on radiation therapy.
After all, Dr Bergfeldt wants to be optimistic. He talks about the possibilities of a Sweden that drives research development and the provided treatments within radiation therapy again. – I want to be able to say that we are once again among the best in the world in this area as a whole, that patients get the absolute best options available and that we develop research environments that create conditions to attract even more research, that lead to more development and even better treatments – in short: an upward facing spiral.
– The number of patients receiving radiation treatment is constantly increasing. However, the number of nurses and doctors who can master the increasingly complex technology and who are doing research in the field is not increasing at the same rate. In order to provide the best treatment, we need to attract more doctors, nurses and medical physicists who are focused on radiation therapy.
So how are we to achieve this?
In the report Swedish radiation therapy loses ground(In Swedish only), which Dr Bergfeldt is one of the authors of, specialized resident physicians, earlier placements with the field of radiation therapy during medical training and targeted marketing is suggested to increase interest. There are also proposals to strengthen the research, to once again be involved in furthering the development. For example, by appointing professors, creating opportunities of employments that allow research to be done half of the time and on top of that engaging funds that are needed to help with the financial aspects.
Photo: Elekta
Dr Bergfeldt is part of a newly started national project that will help future-proof these parts of Swedish radiation therapy. Within the project he will continue to work on some of the report’s suggested actions. – We will focus on supplying the skills needed and making it easier to get the right help in actualizing and implementing the ideas from the research projects. The goal is for Sweden to regain a place among Europe’s leading nations when it comes to research on radiation therapy.
The project includes representatives from different professions, from clinical and academic. Dr Bergfeldt would also like to see the business community involved in developing the research and implementation of radiation therapy and becoming partners who can help test the ideas developed. – Historically, the cooperation between research and industry has been strong in this area. Which is required to produce products that are made available to patients as intended.
A few years ago, I would have said that a vision zero was unattainable. But today, the chances of curing cancer are progressing and getting better.
Well-functioning cooperation is a prerequisite for doing this, Dr Bergfeldt says. And collaborate is exactly what the innovation hub Vision Zero Cancer wants to do. – With Vision Zero Cancer, I’m glad that we have found each other and found forms of cooperating. The way I see it is that there are great conditions for mutually beneficial cooperation. He also welcomes the fact that actors of common interest are pulling in the same direction: that no one should have to die of cancer. – A few years ago, I would have said that a vision zero was unattainable. But today, the chances of curing cancer are progressing and getting better. And in cases where it isn’t curable, the treatments can expand life length and increase the quality of life in the years to be lived.
Better treatment, better lives
We want to find more precise treatment, focusing on the goal and on providing as little side effects as possible. Both during and after treatment. Because it is not just about survival, it is about continuing to live.
HomeVision Zero Cancer becomes host of research network
Vision Zero Cancer becomes host of research network
To transform cancer from a deadly to a curable or chronic disease it is crucial to improve the precision in cancer treatment and follow-up of individual patients’ cancer disease. The Partnership for Precision Medicine in Cancer and Vision Zero Cancer are joining forces to accelerate research into precision medicine, with the aim to benefit every cancer patient.
Partnership for Precision Medicine in Cancer (PPMC) is a network to promote Swedish translational research on precision medicine in cancer. Among other things, this is done through creating better conditions and organization for elevating research.
“We are creating a common way of working in collecting samples and clinical data from cancer patients,” says one of PPMC’s founders Tobias Sjöblom, PhD, Professor and Head, Department of Immunology, Genetics and Pathology at Uppsala University, Director of the Research Infrastructure of Biobank Sweden, BBMRI and Program Director for U-CAN.
Tobias Sjöblom is responsible for the national coordination of the PPMC network. The goal is to be able to include more cancer patients in translational research projects on precision medicine regardless of where in Sweden they live. The aim is also to direct focus externally and find synergies with other actors who share our vision.
To further these goals, Vision Zero Cancer becomes the host for outreach activities and external engagement. Vision Zero Cancer is an innovation milieu Vision Zero Cancer is a Swedish innovation milieu that engages actors across society in strategic actions to work jointly in the mission of eliminating cancer as a cause of death and enable more people to livfe longer and better. As host for PPMC, Vision Zero Cancer will plan and implement outreach activities, develop pathways for connecting other diagnoses in addition to lung cancer to the network and finding models for funding to keep collecting patient samples and enable research.
“We want to stimulate the interest regarding research in precision medicine within industry, healthcare, financiers and patients” says Hans Hägglund, MD, Professor, National Cancer Coordinator and Chairman of Vision Zero Cancer. Research grounded in clinical reality is a step towards no one having to die of cancer.
Together, the two actors will develop a flexible, cross-sectoral and cross-functional model for shared hosting. For seamless integration, Tobias Sjöblom, will become part of the core team at Vision Zero Cancer and the Head of Vision Zero Cancer, Ebba Hallersjö Hult, will become part of the PPMC network’s steering group.
Healthcare has become more and more production oriented. We think that is the wrong way to go. On the one hand, it is difficult for staff to maintain resilient conditions and, on the other hand, the time for research and studies decreases. And research and studies are crucial to developing healthcare and furthering innovation.
HomeProactivity and prevention in achieving the Vision Zero
Proactivity and prevention in achieving the Vision Zero
Improving people’s living habits is a prerequisite for achieving the vision of zero, which is why we gathered a number of actors from different parts of society for a workshop on prevention related to lung cancer.
The aim was clear: to exchange experiences and put organisations and initiatives on the map to find potential cross-border ways of working together in lung cancer prevention. The breadth of knowledge around prevention ranged from smoking, alcohol, environment impact and diet to the means of technology, the challenges of health care, human motivation and politics.
Discussion groups formulated ideas and possible initiatives with the aim of helping to reduce the number of deaths from cancer. A strong need was highlighted in getting more people to quit smoking, fewer young people and school-age children starting out and also seeing how tougher regulation of the tobacco market can be made possible. At the same time, knowledge needs to increase among people about how your surrounding environment, how much you move and what you eat can significantly affect your risks of getting cancer. The meeting agreed that the focus we can direct on prevention issues today in the form of concrete actions and measures will be repaid in both saved lives and financial savings at societal level in the future.
By gathering through a unique point of contact such as Vision Zero cancer, high hopes were expressed to spark a social debate and create the innovation needed to take a holistic approach to cancer prevention and change people’s behavior.
A third of all cancer depend on living habits. This means that one third of all cancers are preventable. And if fewer people get sick, we reduce people’s suffering, increase public health and save society’s resources. The only question is how.
HomeHow lung cancer can be detected and diagnosed earlier in Sweden
How lung cancer can be detected and diagnosed earlier in Sweden
Lung cancer is today the leading cause of death in Sweden. The earlier that lung cancer is detected, the greater are the chances of survival. A national screening programme has been brought to attention, but much needs to be resolved before we are there. Around 70 participants met digitally during a workshop on early detection and diagnosis of lung cancer hosted by Vision Zero cancer. The realization of a national implementation study for a screening program combined with smoking cessation, health informants, lung health checks, biomarkers, advanced imaging, apps and risk assessment tools based on AI in primary care, were some of the ideas that came up.
Lung cancer causes symptoms that come up late in the course of the disease and assessments are complicated. This means that half of the patients have a spread disease at diagnosis. At the same time, the general public and primary care can become better at paying attention to early symptoms, which can easily be confused with other conditions. With new systems and knowledge, we can pick up on symptoms earlier and more quickly come to treatment. And get a better chance of reaching the ‘vision zero’ – that zero people will die as a result of cancer and that more people will live longer and better.
Detecting the cancer in stage 1 gives a two-year survival rate of 80 percent. In stage 4, the two-year survival rate is 10 percent.
The workshop began with insights on why early detection of lung cancer is important, what other countries do on the subject and which needs are prominent in primary care. We were also updated on the expected results of Region Stockholm’s planned pilot study on lung cancer screening in connection with mammography, research on how biomarkers can improve early detection of lung cancer and an exchange of knowledge with the UK. Moderator Lisa Kirsebom interviewed a panel of representatives from health care, government and politics about what is left to solve before a national screening program can become a reality in Sweden.
The participants were then divided into groups to discuss two questions. The first about what data and knowledge we need to foster moving forward. Among other things, the difficulties in finding the right people to screen were highlighted – in the Stockholm region pilot study there are only women, how do we reach men who smoke? And how do we reach newcomers from countries where smoking is more common than in Sweden and where authorities are viewed with scepticism?
– The group that smokes the most can be the hardest to get to participate in screening programs” says one workshop participant. We also need to reach out with information on quitting smoking. Health informants can build trust and find new ways to reach out. Here we can also collect the knowledge generated during this year with covid-19 – how we can overcome the barriers of language and culture.
The group that smokes the most can be the hardest to get to participate in screening programs” says one workshop participant. We also need to reach out with information on quitting smoking.
At the same time, about 15 percent of those who get lung cancer have never smoked. To find them, the health care system, especially within primary care, needs new tools and more support.
The second question regarded in which areas there are needs for strategic and targeted cooperation to detect lung cancer earlier. The discussions led to concrete proposals. An app that combines the patient’s self-perceived symptoms with the geographic presence of radon. The continued strengthened research on radiology and biomarkers were some proposals that came up. Several participants expressed the need and interest to cooperate in the realization of a national implementation study. Allow a number of demonstrative projects where strategies can be tested, some of the workshop participants highlighted e.g. screening, mobile screening, biomarker testing, ways to attract people to screening, collaboration with primary care, digital health surveys, health informants and more general lung health checks.
About 15 percent of those who get lung cancer have never smoked. To find them, the health care system, especially within primary care, needs new tools and more support.
Examples of other ideas highlighted were collaboration with schools/universities/employers both around prevention and early detection, cancer-certified health centres with special expertise on early detection and collaboration between primary care and the country’s diagnostic centre in case of diffuse symptoms.
We are all very aware that something must happen now. I believe a lot in modern technology, algorithms and so forth. And to get information to further this process – that we patients are allowed to record and document symptoms.
The issue of including patients in the development of models, not only via data but also via experience, also came up. The workshop ended with Karin Liljelund, patient representative and vice chairman of the Lung Cancer Association, pointing out that patients would like to share their data. – I appreciate that we patients are invited. We are all very aware that something must happen now. I believe a lot in modern technology, algorithms and so forth. And to get information to further this process – that we patients are allowed to record and document symptoms.
Are you curious about the introductory insights?
The importance of early detection and diagnosis
Mikael Johansson, Associate Professor and Senior Physician Oncology at Norrland University Hospital, talked about the importance of early detection and diagnosis. Over half of all lung cancer cases are diagnosed at stage 4, when the disease is metastatic and incurable. Approximately 25 percent is diagnosed in stages 1 and 2, when it can be treated with surgery or precision radiation therapy. – Detecting the cancer in stage 1 gives a two-year survival rate of 80 percent. In stage 4, the two-year survival rate is 10 percent. Lung cancer screening increases survival, Mikael says. Sweden urgently needs to implement screening of risk groups. But how do we reach them, how do we organize ourselves, how do we choose better audiences?
What does the rest of the world do?
Ebba Hallersjö Hult, Head of the innovation milieu Vision Zero Cancer, gave an outlook on the world. The United States and South Korea have introduced targeted screening programs. Canada and China also carry out studies and plans towards this. The UK has conducted several studies and tested strategies to find and reach the right people. In Norway, an implementation study will start in 2021 in which approximately 1,000 high-risk people will be screened. The focus is to build knowledge about cost-effectiveness of lung cancer screening. Denmark is considering launching a small-scale screening program to map the impact on capacity needs in subsequent diagnostics. There too is a big ongoing discussion about how best to reach the risk group. In the EU, Croatia, a high-incidence country, has begun implementation. Also underway are a lot of exiting steps taken in the EU within the study 4-IN-THE-LUNG-RUN. The Study, within the Horizon 2020 programme, evaluates different strategies for lung cancer screening in 2020-2024. The study involves medical research institutions from Holland, Germany, England, France, Spain and Italy. – Sweden is timely with discussions, research and studies. Now is the time to take it further, Ebba concludes.
Decision support in primary care to detect lung cancer earlier
It is a challenge to find patients who have cancer among all those who seek medical treatment within primary care, says Elinor Nemlander, General Practitioner at Sophiahemmet Primary Care Center and PhD student at Karolinska Institutet. In primary care, symptoms that may exist due to cancer are common. Coughing is the fourth most common cause for visiting. Elinor Nemlander believes in risk assessment tools, which can help primary care detect the right patients. For this, primary care-based clinical research is needed on the predictive value of symptoms, which is exactly the research that Elinor is undertaking.
Pilot study and cost-effectiveness of lung cancer screening in conjunction with mammography
Screening can require significant resources if the precision in the selection of people to screen is not accurate. The Stockholm-Gotland region has investigated the interest in and cost-effectiveness of lung cancer screening. In the pilot project, 1,727 women were asked questions about smoking habits and health at their mammography screening. 90% said they were also interested in lung cancer screening. Based on this, IHE calculated that lung cancer screening is cost-effective and lowers the mortality rate of patients 55-74 years of age. Telling us about this was Gunnar Wagenius, Senior Physician at Karolinska University Hospital and Chairman of the National Lung Cancer Registry, and Katarina Steen Carlsson, Associate Professor of Health Economics at Lund University and IHE.
Conclusions from expert meeting with England on lung cancer screening
Suzanne Håkansson, Senior Director Government Affairs, AstraZeneca AB and a member of Vision Zero Cancer’s core team shared words on a meeting and knowledge exchange held with British experts which Vision Zero cancer arranged earlier this autumn. Last year, the UK launched its Long-Term Cancer Plan, with a couple of quantitative targets. The NHS has encouraged development projects to contribute to the objectives. Here you will find more about the UK’s success factors for lung cancer screening.
Biomarkers to improve early detection of lung cancer
Mattias Johansson, PhD, Scientist, Genetic Epidemiology Group at the International Agency for Research on Cancer (IARC), talked about his research on how biomarkers can improve CT lung cancer screening. After a long study including 1 200 proteins, he and the research team have scaled down the work to seven biomarkers. These can significantly improve prediction, compared to a standard risk model based on smoking data. The study is ongoing. – Next year we will try to validate the panel. In a year and a half, we hope that we will have a usable tool to really improve the inclusion criteria and follow-up process.
Panel discussions on issues left to solve and what obstacles to overcome
After the introductory talks, the moderator Lisa Kirsebom, science journalist and natural scientist, interviewed a panel consisting of Jan Nyman, Associate Professor andSenior physician Oncology at Sahlgrenska University Hospital and Chairman of the National Working Group for Lung Cancer, Mattias Fredriksson, Head of Unit responsible for national guidelines and screening at the National Board of Health and Welfare from the National Board of Health and Welfare, Jan Adolfsson, Associate Professor and Physician, Member of the National Screening Council and Camilla Waltersson Grönvall, Member of Parliament, Ordinary member of the Committee on Health and Welfare and spokesperson for the party Moderaterna.
Jan Nyman opens the discussion with stating that the screening population is set – 55-74-year-olds who are or have been heavy smokers. The question is now rather how to get them to come to screening. Mattias points out that other screening programs are often aimed at people who can be found using social security numbers. But now it is a group with a risk behaviour we need to find, they are not a given part of the population. In addition, about 15 percent of patients with lung cancer have never smoked. To find them, there must be other ways than screening.
Another aspect of establishing a screening program is how long it takes. Jan Adolfsson points out that the road to a national screening program is long. He compares it to mammography screening, which took 7-8 years to set up, and colorectal cancer screening, where the recommendation came in 2012 but implementation has not yet happened in many regions. From a political point of view, Camilla Waltersson Grönvall wants to see solutions move faster. For example, through more pilot studies, which Mattias Fredriksson welcomes. All initiatives are valuable and teach us more which moves us further towards making a final decision, he says.
Jan Adolfsson emphasizes that it is possible to start with efforts aimed at quitting smoking right away. And that it is the most cost-effective solution. At the same time, efforts are not mutually exclusive and can with advantage take place in parallel.
The panel agrees that the national perspective is important. Both for pilot studies, tools in primary care and for the possible screening recommendation.
How do we detect cancer earlier?
The earlier cancer is detected, the greater the chances of survival. With new systems and knowledge, we can catch up on symptoms earlier and more quickly come to treatment. And get more chances to reach the vision of zero persons dying from cancer and more people living longer and better.
HomeGP’s and PhD students – Elinor and Eliya are looking for ways to detect cancer earlier
GP’s and PhD students – Elinor and Eliya are looking for ways to detect cancer earlier
Coughing does not have to mean the same thing in primary care as in the office of the pulmonary oncologist. Research on cancer, and the standardised care pathways, are mostly based on set diagnoses and are mainly based on research done in secondary care. This became clear to General Practitioners Elinor Nemlander and Eliya Abedi – Sweden needs more primary care-focused research, based on symptoms and not diagnoses.
Eliya Abedi and Elinor Nemlander
For almost every cancer diagnosis Sweden has a national standardized care pathway: what assessments should be done, what treatment can be given and a time frame for the time allowed to pass between suspicion and treatment. After its introduction in 2015, the expected impact in primary care was delayed. Perhaps precisely because the care pathway is based on diagnoses. – Patients come to primary care with symptoms – not diagnoses, says Elinor Nemlander. If you cough at a pulmonary oncological clinic, the probability that the cough is due to lung cancer is quite large. Coughing is one of the most frequently diagnosed symptoms in primary care, but a GP doesn’t even see one new lung cancer patient a year. It is not always the case that symptoms that are predictive of cancer in secondary care are equally predictive of cancer in primary care.
Patients come to primary care with symptoms – not diagnoses.
Elinor and Eliya have been working since 2017 with adapting the standardized care pathways and educating health care personnel as part of the knowledge team CaPrim – an abbreviation of cancer in primary care. CaPrim is part of Academic Primary Care Center – a joint venture between Stockholm Health Care Region, Karolinska Institutet and other partners for education, research and development for students and healthcare professionals working in primary care.
Earlier this year, Elinor and Eliya were enrolled as PhD students at Karolinska Institutet. They will research on precisely how cancer can be detected earlier in primary care. Elinor’s focus is on what symptoms may indicate cancer. – The research so far has largely looked back at patients with cancer diagnosis in secondary care and what symptoms they had before diagnosis. But there is limited research on those seeking for the same symptoms in primary care. For example, how predictive is anemia for cancer in primary care?
Elinor will also investigate combinations of factors that may indicate lung cancer in patients who have never smoked. These may include factors such as symptoms, findings during assessments, lifestyle and other diagnosed disease. Finding the right combinations is crucial. – We should not fail to detect those who have cancer, but we cannot investigate everyone with symptoms. There are also risks associated with over-investigation, such as unnecessary anxiety for the patient, neglect of other possible care and increased costs of care. We need to find ways to detect the right people to further assess. This can be done with IT support and risk assessment tools which, for example, could find the combinations that increase the risk of cancer.
We should not fail to detect those who have cancer, but we cannot investigate everyone with symptoms.
When it comes to risk assessment tools, the UK often comes up as an example. – Unfortunately their health care system is divided in a different way than ours, so we can’t use their model outright. Much of what is done in primary care here is done in secondary care there. Eliya will do more research on risk assessment tools, looking specifically at colorectal cancer.
In Sweden, between 70 and 85 percent of patients, who later turn out to have cancer, start their investigation within primary care. But often it takes a long time and numerous visits before the diagnosis is made. Most reports of diagnostic errors related to primary care regard delayed or lack of cancer diagnosis. – Eliya will look at whether an increased number of visits to primary care in a short period of time is predictive of cancer.
Elinor and Eliya spend half of their time on their PdD positions. The other half of their working hours, they work as general practitioners. – This means that we have contact with the operational work on the floor in a different way, that we are clinically active. We hope that our research can contribute with scientific input to risk assessment tools that we and our colleagues can then use in our daily work.
Why has there been so little research in primary care so far? Elinor believes it is due to a lack of economic preconditions and time. The proportion of research funding going to primary care is small. There’s so much to do at the clinic that it’s hard to keep up with anything else. And also the very breadth of topics to target. It is not easy to find someone who works in primary care, who wants to do research and is interested in cancer. – Actually, I ended up here mostly by accident. It started with my being involved in management work during my duties as specialist. That’s where I was recruited into CaPrim. That I chose to start researching was because of CaPrim. It became clear that this is research that is lacking and needed.
How do we detect cancer earlier?
The earlier cancer is detected, the greater the chances of survival. With new systems and knowledge, we can catch up on symptoms earlier and more quickly come to treatment. And get more chances to reach the vision of zero persons dying from cancer and more people living longer and better.
HomeFor Mia, the diagnosis became a drive to make care better
For Mia, the diagnosis became a drive to make care better
Fourteen. That’s how many times, Mia Rajalin visited primary care before she received the chest X-ray that showed the tumor. And the X-ray referral was sent with hesitation – she was too young and had never smoked a cigarette.
Photographer Petra Kyllerman
The diagnosis became drive and commitment. Mia wants to work so that no one else suffers from what she, and many others, have gone through. To not receive a diagnos in primary care even though you yourself suspect that you are sick. Mia’s 14 visits occurred over a period of one and a half years. One difficulty in detecting lung cancer, which Mia was diagnosed with, is that the first symptoms are so common. Cough, fatigue, pain. However, visiting primary care so often in such a short period of time, that is not common. – I felt dismissed many times. Before this, I had hardly ever sought medical attention.
The whole society would benefit from early detection. People of working age can continue to work, loved ones feel good, children do not have to undergo the trauma of losing a parent to cancer.
Mia believes that there is an acceptance of the low proportion of lung cancer cases detected in stage one and two. You’ve gotten used to it, you see it as a silent cancer. Most often, the care system detects the cancer in stage four when it is not curable. But patients report symptoms long before they are diagnosed. Many lives can be saved, and early detection would also have other positive effects. – The whole society would benefit from it. People of working age can continue to work, loved ones feel good, children do not have to undergo the trauma of losing a parent to cancer. And the cost of care of course – the new treatments are good, but expensive. If it is possible to operate more in stage one and two, that would be half the cost.
Artificial intelligence could detect whether a patient has sought care several times in a short time. It can help to see changes in the visiting pattern, where the various symptoms altogether can point towards cancer.
At the same time, Mia points out that shortcomings are in the structure and not in competence. To only get 10 minutes per patient, not have time to read medical records, learn that smoking is the only cause. Then, of course, cancer cannot be the first suspicion when a patient comes in and is tired. What is needed is supportive tools. She lists examples used by other countries. As risk assessment tools, screening, and symptom checkers. – It’s pretty simple stuff, which would go pretty quick to put in. I myself filled out a symptom checker with all the symptoms I had before the diagnosis. The result was that it is something, and it could be these diseases. Lung cancer was on that list. Mia also talks about the possibilities of digital tools. – For example, artificial intelligence could detect whether a patient has sought care several times in a short time. It can help to see changes in the visiting pattern, where the various symptoms altogether can point towards cancer.
Vision Zero Cancer can work cross-border and convey conversations without anything being sensitive, where the common goal is what matters. They have a unique position as a spider in the web.
Two of Mia’s engagements are the Lung Cancer Association and Vision Zero Cancer, where she is part of the core team as a patient representative. – I have a foot in both worlds because I myself work in health care. I can understand the problems of care but also see that the patient’s needs have to be better met. It should not take 14 visits before the detection of lung cancer. Healthcare needs to be given more time with the patient and systemic support support.
She sees one of the benefits of Vision Zero Cancer as being a neutral forum. – Vision Zero Cancer can work cross-border and convey conversations without anything being sensitive, where the common goal is what matters. They have a unique position as a spider in the web. They can make sure it’s a collaboration. Because that is what it needs to be.
How do we detect cancer earlier?
The earlier cancer is detected, the greater are the chances of survival. With new systems and knowledge, we can pick up on symptoms earlier and more quickly come to treatment. And get better chances to reach vision zero.
This website uses cookies to improve your experience while you navigate through the website. Out of these cookies, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may have an effect on your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. This category only includes cookies that ensures basic functionalities and security features of the website. These cookies do not store any personal information.
Any cookies that may not be particularly necessary for the website to function and is used specifically to collect user personal data via analytics, ads, other embedded contents are termed as non-necessary cookies. It is mandatory to procure user consent prior to running these cookies on your website.